Article Text

Abstract
The consequences of vitamin D and dietary calcium deficiency have become a huge public health concern in the UK. The burden of disease from these deficiencies includes rickets, and hypocalcaemic seizures, dilated cardiomyopathy and mostly occult myopathy and osteomalacia. The increasing burden of the disease is intrinsically linked to ethnicity and the population demographic changes in the UK. Three facts have led to the resurfacing of the English disease: (1) the UK has no ultraviolet sunlight for at least 6 months of the year, (2) dark skin produces far less vitamin D than white skin per unit ultraviolet light exposure, and (3) non-European Union immigration over the last century. To date, the UK government demonstrates incomplete understanding of these three facts, and its failure to adjust its prevention programmes to changing demographics is endangering the health and life of UK residents with dark skin, of whom infants are the most vulnerable. Establishing accountability through the implementation of monitored antenatal and infantile supplementation programmes and mandatory food fortification is overdue.
- immigration
- dark skin
- South Asian
- African
- vitamin D deficiency
Statistics from Altmetric.com
Introduction
Quite in contrast to their continental European counterparts, paediatric Accident and Emergency doctors in the UK often encounter dark-skinned infants with hypocalcaemic seizures, hypocalcaemic cardiomyopathy and rickets during winter and spring. This article will explain the critical role of the UK government in the causation and prevention of what was once called, and still is, the ‘English disease’.
Rickets and osteomalacia occur due to defective mineralisation of hypertrophic growth plate chondrocytes and preformed osteoid in existing bone, respectively. In children, rickets and osteomalacia always coexist. The most common cause of rickets and osteomalacia worldwide is calcium deprivation, secondary to low dietary calcium (‘nutritional’) and/or low ultraviolet B (UVB) sunlight exposure,1 the main source of cutaneous vitamin D production (‘solar’).2 There is very little vitamin D in diet (including breast milk) and thus humans are mainly dependent on solar UVB for vitamin D supply. Cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2) undergo hepatic 25-hydroxylation to form calcidiol or 25 hydroxyvitamin D (25OHD, stable form reflecting vitamin D status), and then renal 1-hydroxylation to form the hormone calcitriol or 1,25 dihydroxyvitamin D. In contrast to calcitriol, vitamin D and 25OHD are biologically inert. The main action of calcitriol is to aid intestinal calcium absorption. When dietary calcium or solar vitamin D availability is low, secondary hyperparathyroidism sets in, which increases intestinal calcium absorption and bone resorption in the short term to maintain normal serum calcium concentrations. Unopposed, this compensation will fail in the long term and hyperparathyroidism-induced renal phosphate wasting will lead to hypophosphataemia, which ultimately impairs mineralisation on the tissue level causing rickets and osteomalacia.3 Hypocalcaemic complications of calcium deprivation can occur before these hypophosphataemic complications, especially during phases of rapid growth, that is, during infancy and adolescence.4 5
Dietary calcium deficiency rickets (due to nutritional deficits) prevails in low-income countries, whereas vitamin D deficiency rickets (due to reduced solar UVB exposure/latitude) predominates in high-income countries.3 Calcium deprivation and all its hypocalcaemic or hypophosphataemic complications can be easily prevented by ensuring adequate calcium and vitamin D supply.6 Factors causing vitamin D deficiency in high-income countries such as the UK specifically include the following:
Latitude: lack of UVB radiation for at least 6 months of the year due to its geographical location.2 7
Ethnicity: dark skin (Fitzpatrick skin type IV (light brown), V (dark brown) and VI (black)) massively reduces cutaneous synthesis of vitamin D.7
Culture: covered clothing, low dietary vitamin D and calcium intake.3 8
Sunscreen: excessive use of sunscreen9 due to fear of skin cancer.
It is not difficult to see that the majority of the above factors are non-modifiable. Therefore, supplementation or food fortification with vitamin D is necessary to prevent rickets and osteomalacia in an ethnically and culturally increasingly diverse society. Non-European Union (EU) immigration over the last century has led to a change in population demographics, with a growing proportion of the resident population (14% in the 2011 census) being dark-skinned (figure 1).10 Whole body clothing for cultural, medical or other reasons further reduces sunlight exposure. These high-risk groups are unable to produce sufficient vitamin D in the UK. Unfortunately, the UK has not adapted to its ethnic and cultural diversity, which has led to a resurgence in rickets11 and hypocalcaemic complications,5 a problem further augmented by a lack of mandatory food fortification12 and a complex and poorly implemented infant vitamin D supplementation policy.13

Census data (1991–2011) demonstrating an upward trend in the proportion of non-white population and a downward trend in the proportion of white population. Data from national statistics.10
Burden of disease from vitamin D deficiency and rickets in the UK
‘Nutritional’ rickets was indeed originally caused by poor nutrition but was always also of ‘solar’ origin due to pollution during the industrial revolution. The fact that the English disease has resurfaced as a major public health problem in the UK in the last 50 years, however, is much less ‘nutritional’, but due to the increase in the ethnic high-risk proportion of the population. Over the past few decades, several UK studies have highlighted the increasing burden of rickets5 11 14–16 and the increased susceptibility of the Black, Asian and Minority Ethnic (BAME) groups. The burden of disease from solar vitamin D and dietary calcium deficiency is much wider and goes beyond the bone pathology. The British Paediatric Surveillance Unit survey (September 2011–2013) reported a total of 91 cases (85%, n=77 were infants) of hypocalcaemic seizures due to vitamin D deficiency, amounting to an annual incidence of 3.49 per million children (0–15 years), with the highest incidence in the South Asian population at 26.04 per million.5 In contrast to the white population, its high incidence in the BAME population precludes rickets from being classified as a rare disease (table 1).16 A retrospective study from South-East England identified 16 BAME cases (6 Asian, 10 black) of hypocalcaemic dilated cardiomyopathy secondary to severe vitamin D deficiency between 2000 and 2006.17 These cases displayed significant mortality (n=3) and morbidity requiring mechanical ventilatory and circulatory support (n=2 each) and referral for cardiac transplantation (n=2).17 In a postmortem study from London (n=52), hypocalcaemia due to vitamin D deficiency was considered accountable for death in three BAME children; they all showed radiological and histological rickets: two babies had cardiomyopathy and a 3-year-old had hypocalcaemic seizures.18 These reports are not collections of tragic medical rarities. Infants presenting with complications of hypocalcaemia such as seizures,4 5 11 dilated cardiomyopathy,17 cardiac death18 and overt rickets14 19 only represent the tip of the iceberg of a public health crisis. The extent of hidden pathology remains unknown. Histological changes of rickets and osteomalacia occur long before the disease becomes evident on radiographs.3 One way to gain insight into the widespread prevalence of rickets and osteomalacia in the UK is from postmortem studies,18 which demonstrate histological changes in nearly 70% of infants studied, which however were not quantified. Osteomalacia in adults on postmortem examination is also highly prevalent (nearly 25% of a low-risk population studied, n=675) in northern Europe.20
Rickets overall is a rare disease in high-income countries.
The increased prevalence of rickets in the immigrant and resident BAME population in the UK, especially the South Asian community, is not new knowledge and was noted as far back as the 1960s,21 when the UK government commonly referred to it as the ‘Asian rickets’.22 Although immigration of dark-skinned individuals has contributed to the rise in rickets in most developed countries,16 23 an additional contributing factor in the UK is its geographical location24 and possibly the changing climate.25 Hence, vitamin D deficiency is neither limited to the winter months nor exclusive to BAME population. A study from Manchester reported a median serum 25OHD concentrations in summer of 28.6 nmol/L (IQR 21.3–41.6), falling further to 18.4 nmol/L (IQR 12.7–25.7) in winter in adult residents of South Asian origin.8 These findings were resonated in another study in women of childbearing age, where severe deficiency (25OHD<25 nmol/L) was prevalent in 81% and 79.2% of UK South Asians in winter and autumn, respectively.26 In a study of white women from North-West England (n=333), 27% and 7% had insufficient (<50 nmol/L) and deficient (<25 nmol/L) serum 25OHD levels during pregnancy, and 48% and 11% 4 months postdelivery, respectively.27 The median 25OHD in cord blood samples was only 50% of maternal 25OHD levels, and the prevalence of deficiency and insufficiency in infants at 4 months (n=322) was 13% and 24%, respectively.27 No UK study compared vitamin D levels in native and migrant mother–baby pairs, but an Italian study showed that severe vitamin D deficiency (25OHD<25 nmol/L) was widely prevalent in the migrant mothers and their newborns (48.4% and 76.2%, respectively) when compared with natives (38% and 18%, respectively).28
The UK National Diet and Nutrition Survey found that the mean intake of vitamin D was below the reference nutrient intake: only 29% for children aged 1.5–3 years and 33% for adults ≥65 years, and nearly a fifth of all subjects studied were vitamin D-deficient (25OHD<25 nmol/L).29
Although vitamin D deficiency is pandemic in Europe, it is more prevalent in some mid-latitude countries including the UK when compared with northerly latitude countries such as Norway, Iceland or Finland even after accounting for ethnicity.30 The lower prevalence in the northern latitude is attributed to better supplementation policies and also food fortification.30
Factors contributing to resurgence of rickets in the UK
The increasing BAME resident and immigrant population
A question on ethnic group was first introduced in the 1991 census ‘to enable monitoring for equal opportunities/anti discrimination policies’ and ‘to plan for the future through resource allocation and provision of services’.10 However, this does not seem to have happened in relation to rickets prevention despite the so obviously increasing proportion of dark-skinned individuals. The most recent census (2011) reported that 14% of the population in England and Wales are of BAME origin, which is a significant rise from previous census in 2001 (8.7%) and 1991 (5.9%) (figure 1).10 Every year, nearly 13% of babies born in England and Wales have been of BAME background since 2014,10 and around 100 000–150 000 people of BAME background (net) are added to the UK population through immigration (figure 2).10 Therefore, the government needs to adjust its healthcare systems to these population demographic changes.

UK net migration data over the last decade demonstrating an increase in the number of people with dark skin living in the UK. There has been a negative net migration of the white British population and a positive net migration in the BAME population. BAME net migration was derived from national statistics data summarising the following non-EU global regions of origin/destination: BAME=net Asian migrants+net rest of the world migrants (Sub-Saharan and North Africa, Central and South America, Oceania, excluding North American migrants).10 The assumption was made that migrants from/to EU and North America are exclusively white, and from/to BAME global regions are exclusively dark-skinned. Net total migration (grey bar) equals net BAME (black bar)+net white British (white bar)+net North America+net EU migration. EU, European Union; BAME, Black, Asian and Minority Ethnic.
A multitude of factors contribute to the increased prevalence of vitamin D deficiency in BAME groups residing in high-latitude countries. An adult study of South Asian residents in Manchester reported lower oral intake of dietary vitamin D (mean of 1.32 µg compared with 3.26 µg in white subjects), sun avoidance when outside and lower amounts of skin surface exposure.8 However by far the greatest contributing factor is reduced skin synthesis of vitamin D.7 Dark skin, when compared with white skin, requires much greater exposure to sunlight to improve circulating 25OHD levels as melanin absorbs a substantial proportion of the UVB light.7 Hence, even the UK-recommended summer sunlight exposure amounts fail to produce sufficient circulating 25OHD in the dark-skinned population.7 Lack of ethnicity-specific guidance on sunlight exposure,7 minimal impact of dietary vitamin D in improving serum 25OHD levels26 and poor supplementation policies in infants13 and pregnant women all contribute to widespread vitamin D deficiency in dark-skinned individuals, all year round.26
UK politics and policy: from success to failure
There is an interesting history behind the increasing burden of rickets in the UK. During World War II, Britain triumphed eradication of rickets through rationing, food fortification and supplementation of infants and pregnant women with cod-liver oil. Strangely, the same country which once demonstrated the effectiveness of good public health policies is now struggling to tackle this easily preventable disease. In the 1950s, uncontrolled fortification of infant formula and food (4000 IU/day, which is 10 times the current recommended dose of 400 IU/day) was implicated in the causation of infantile hypercalcaemia,31 which led the government to withdraw fortification. Ever since this time, the ‘English disease’ has returned to the UK to the extent that today, Britain serves as an example of how lack of effective policy implementation can lead to a rise in a preventable disease such as rickets. Rickets or ‘Asian rickets’ has enormous political significance and has been the subject of debate in parliament since the 1960s.22 There is a suggestion that the resurgence of rickets symbolises socioeconomic inequality and racial or ethnic health disparity in the UK, which is discussed in detail elsewhere.22 The government continues to shy away from the issue. The senior author submitted a parliamentary question to the House of Lords in November 2017, with evidence demonstrating the ineffectiveness of the UK’s infant vitamin D supplementation programme13 and queried the government’s future plans to prevent rickets in the UK. The response, detailed in table 2, reflects the government’s current misconceptions.
Parliamentary response to future plans on rickets prevention in the UK, which demonstrates serious misconceptions and incomplete knowledge of evidence (available from http://www.parliament.uk/business/publications/written-questions-answers-statements/written-question/Lords/2017-11-13/HL3098/)
The UK prevention programme: complex, outdated, unmonitored, ineffective
The Scientific Advisory Committee on Nutrition (SACN) sets vitamin D ‘reference nutrient intake’ for adults and children aged >4 years (10 µg or 400 IU/day) and ‘safe intake’ for infants (8.5–10 µg or 340–400 IU/day) and children aged 1–4 years (10 µg or 400 IU/day).32 The SACN does not recommend supplements or food fortification but acknowledges the difficulty of achieving the recommended intakes from natural food sources and advised the government to consider strategies for the UK population to achieve the above intake.32 While most authorities consider optimal levels of serum 25OHD to be above 50 nmol/L,6 the SACN recommends that levels should not fall below 25 nmol/L.32 The National Institute for Health and Care Excellence makes certain recommendations to multiple agencies (including the Department of Health, Public Health England and healthcare professionals) to increase supplement use in at-risk populations.33 Based on the latest SACN vitamin D and health report,32 Public Health England recommends that populations at risk should take supplements containing 10 µg (400 IU) of vitamin D all year round (https://www.gov.uk/government/news/phe-publishes-new-advice-on-vitamin-d). The recommendation for infants and children however is overly complex (table 3) and now outdated in relation to formula feeding and dose for children >1 year. The evidence-based global consensus on the prevention of nutritional rickets recommends universal supplementation of all infants,6 which is followed by most European countries (85%, n=24/29).13 SACN does not recommend vitamin D supplements for formula-fed infants, while new evidence demonstrates that formula feeding does not protect from rickets.5 6 In the British Paediatric Surveillance Unit survey, 19% (n=15/77) of infants presenting with hypocalcaemic seizures were exclusively formula-fed and 9% (n=7) received mixed breast and formula feed.5
UK supplementation policy in comparison with global consensus recommendation
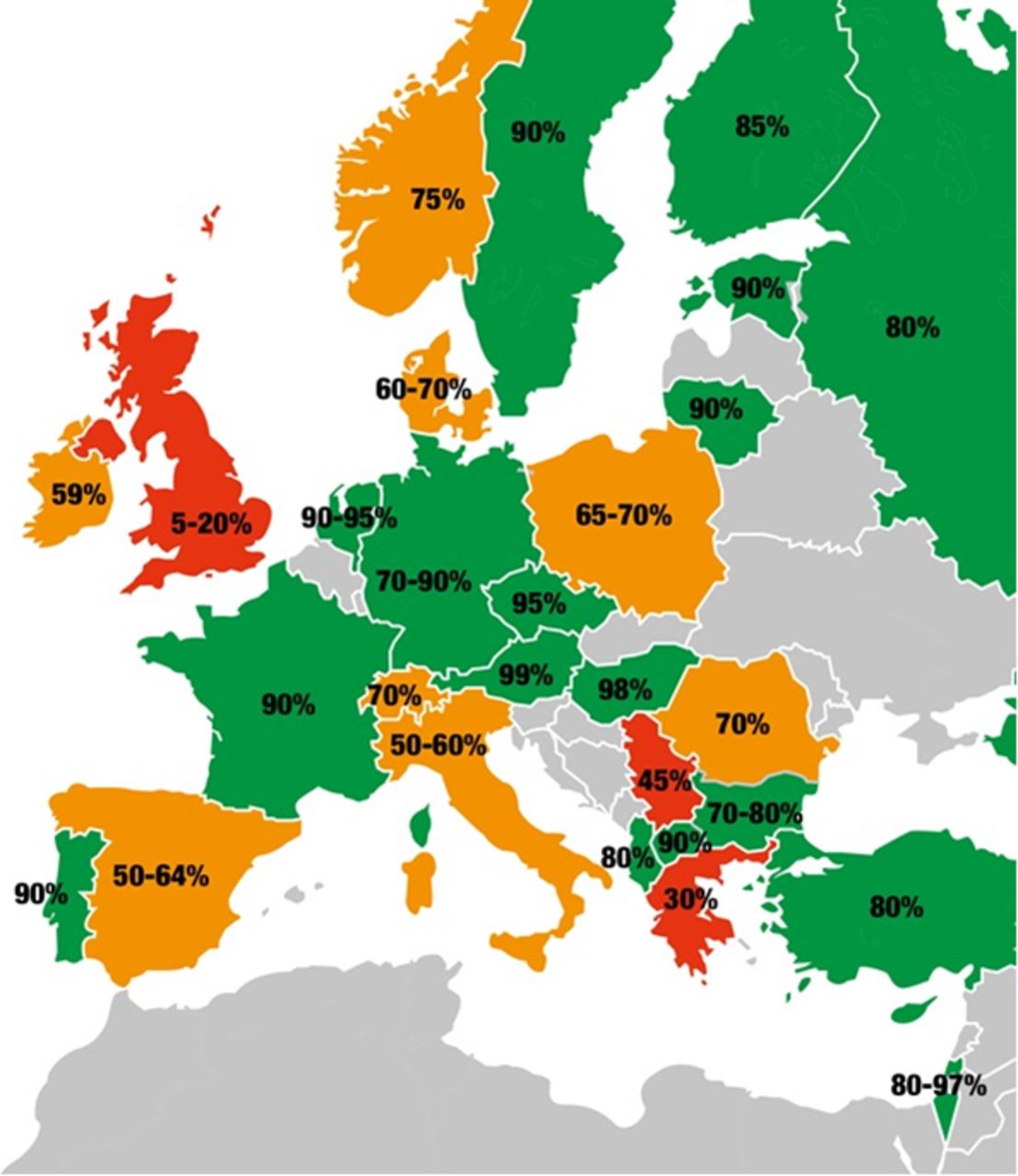
In contrast to the global consensus recommendation (10 µg or 400 IU for infants and 15 µg or 600 IU for children >1 year), SACN and Public Health England recommend 8.5–10 µg of vitamin D for infants and children and the government supplies Healthy Start vitamins, which only provide 7.5 µg. The operation of the Healthy Start scheme, which provides free vitamins to low-income families, is also very complex,34 leading to low uptake, poor accessibility and lack of motivation to take daily supplements,35 not to mention the lack of parental awareness.36 Apart from the complexity of the guidance, it is mainly the complete lack of accountability and monitoring that is responsible for the failing of the Healthy Start programme to improve the vitamin D status of the at-risk population.34 The UK’s unmonitored infant vitamin D supplementation programme has the lowest adherence rate in Europe, with just 5%–20% of infants actually receiving vitamin D drops (figure 3).13
{kind=link}
{kind=link}
{kind=link}
Adherence rates for infant vitamin D supplementation in the first year of life in Europe, with UK reporting the lowest rates.13 Good adherence (≥80% of infants supplemented) is indicated in green, moderate adherence (79%–50%) in orange and low adherence (<50%) in red.
Preventative strategies
Given the low uptake of supplements, the long-term solution to vitamin D deficiency is mandatory food fortification,12 which has been successfully implemented in countries such as Canada. However, this may not be easily adopted by the UK government given that it also shies away from adopting folic acid fortification despite overwhelming evidence on its role in preventing neural tube defects.37 Mandatory fortification of flour with folic acid is adopted by 78 countries but not the UK, which has resulted in a continued rise in neural tube defects in the UK.37 Countries with mandatory folic acid fortification have seen a decline in neural tube defects compared with those with voluntary or no fortification.38 Despite SACN recommendation to adopt mandatory folic acid fortification of flour (in 2006 and 2009), the UK government has not taken any positive steps. Not surprisingly in 2017, Food Standards Scotland requested SACN to provide advice on whether its previous recommendations on mandatory fortification still apply, with an intention to proceed unilaterally.39 Similarly, iodine deficiency, which is considered the single most important preventable cause of brain damage by the WHO, is thought to be re-emerging as a public health concern in the UK due to lack of national salt iodisation and monitoring of iodine levels in pregnancy.40
While mandatory food fortification may be the best long-term solution to improve the vitamin D status at a population level,12 certain measures in the interim are crucial in protecting the most vulnerable group—infants. As most infants acquire vitamin D deficiency from the mother, it is equally important to ensure adequate supplementation during pregnancy and to start infant supplementation at birth. Success of supplementation policies requires that authorities adopt multiple, simple strategies. We have previously compared vitamin D supplementation policies across Europe and determined that the following policy implementation features were significantly associated with improved adherence in the first year of life: universal supplementation independent of feeding mode (p=0.007), providing information on supplementation at discharge from neonatal units (p=0.02), providing financial family support (p=0.005) and monitoring adherence at child health surveillance visits (p=0.001).13 The UK currently does not adopt any of the above features, except providing financial support only to low-income families.
Public health policies need to be simple to work. Universal supplementation of all infants6 enhances adherence13; moreover, formula feeds do not protect the infant from rickets5 6 and hence the SACN guidance requires updating and simplifying. Most importantly, similar to the vaccination programme, a group of healthcare professionals need to be made responsible for delivering this prevention programme, in the same way as the vaccination programme. In the authors’ point of view, establishing accountability is the most essential change required in the UK.
Based on data from the European survey,13 the suggested responsibilities are as follows:
Healthcare professionals providing antenatal care include monitoring of supplementation at every routine visit.
Neonatal units provide specific information on prevention programmes to parents, commence vitamin D supplementation at birth and provide first bottle at discharge.
On registration at the general practice, adherence to vitamin D supplementation is checked and then monitored at every single vaccination time point and red book visit.
Inclusion of a monitoring question on adherence to vitamin D supplements in maternity notes and personal child health record (red book), at all routine time points, which reminds healthcare professionals and parents.
The government should provide financial remuneration to GPs delivering this prevention programme in a similar way as for the immunisation programme (prevention of infections). The government should consider linking financial family support to adherence to all prevention programmes.
Future considerations
The majority of the European medical literature on rickets and hypocalcaemic complications comes from the UK.1 Current studies are mainly based on clinical presentation or serum 25OHD measurements. Further research is required to explore the true burden of rickets and specifically osteomalacia in the UK. Histological changes occur long before the disease becomes clinically, biochemically or radiologically evident.3 Therefore, the true prevalence of occult rickets and osteomalacia can only be identified by quantitative growth plate histology and bone histomorphometry. These investigations are invasive in alive children or adults but can be undertaken during postmortem examination.
Taking daily vitamin D supplements prevents rickets but may pose an issue with adherence, similar to folic acid supplementation, especially if unmonitored. However, vitamin D can also be easily and safely administered in bolus doses, alleviating the need for daily supplementation and parental compliance. Licensed preparations for bolus administration are readily available in the UK. Feasibility of administering bolus doses of vitamin D during immunisations and routine child care visits in the UK should be explored. Likewise, safety and feasibility of administering bolus doses of vitamin D during antenatal visits should also be explored.
The increasing UK BAME population requires lifelong supplementation. Since this can never be delivered, food fortification is the obvious solution to the problem. Further studies are required to bridge the gap in knowledge required to facilitate food fortification, and to compare the cost-effectiveness of fortification and supplementation programmes.
Conclusions
The UK population is more ethnically and culturally diverse than ever. The increasing UK BAME population is fully exposed to the complications of vitamin D deficiency due to their dark skin and cultural traditions. The UK government demonstrates serious misconception of the actual public health issue and the implementation of effective prevention programmes, and an astounding ignorance of changing population demographics. National statistics demonstrate a constant rise of the UK BAME resident population through continued non-EU immigration from countries with predominantly dark-skinned population (Asia, Africa), with high birth rates. We call for the government to consider adaptation of their public health policy implementation strategy and introduce accountability through monitoring.
References
Footnotes
Contributors SU: preparation of the manuscript and final approval. WH: concept, intellectual revision and final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.