Article Text

Abstract
Background Treatment based on ultrasound (US) and colour Doppler (CD) findings in midportion Achilles tendinosis has shown promising results. In a randomised study on a small patient material, similar short-term clinical results were demonstrated with surgery outside the tendon and sclerosing polidocanol injections, but surgical treatment led to a faster return to activity.
Objective To evaluate the clinical results of US and CD-guided mini-surgery (scraping) outside the ventral tendon in a larger patient material and, in a randomised study, compare two different techniques for surgical scraping.
Material and methods 103 patients (66 men, 37 women), mean age 43 years (range 24–77), with midportion tendinosis in 125 Achilles tendons were included. Patients from a large group (88 tendons), and a randomised study (37 tendons), were in local anaesthesia treated with a US and CD-guided new surgical approach outside the ventral tendon. All patients in the large group, and one arm of the randomised study, were treated open with a scalpel, while the other arm of the randomised study were treated percutaneously. Pain during Achilles tendon loading activity (Visual Analogue Scale (VAS)), and satisfaction with treatment, were evaluated.
Results Before surgery, the mean VAS was 73. After surgery (follow-up mean 18 months, range 6–33), the mean VAS was 3 in 111 tendons (89%) from satisfied patients back in full Achilles tendon loading activity. In the randomised study, there were no significant differences in the results between open treatment with a scalpel and percutaneous treatment with a needle.
Conclusions US and CD-guided scraping show good short-term results in midportion Achilles tendinosis.
Statistics from Altmetric.com
Introduction
Treatment of the chronic painful Achilles midportion has undergone radical changes during the last 10 years. Painful eccentric calf muscle training and ultrasound (US) and Doppler-guided sclerosing polidocanol injections have shown good clinical results,1,–,3 and there has been less need to use the traditional intratendinous surgical approaches. The traditional surgical treatment of midportion Achilles tendinosis has for many years consisted of a dorsal approach, with a central longitudinal tenotomy and excision of tendinosis tissue.4,–,6 This method is associated with a relatively long postoperative rehabilitation, and often it takes 3–6 months before the patients are back in full tendon-loading activity.7 A pilot study using a US+Doppler-guided ‘scraping’ technique, combined with a short rehabilitation period, showed promising results.8 The ‘scraping’ technique is based on the same findings that started the sclerosing polidocanol injection treatment, where grey-scale US and Doppler12 13 demonstrated a relationship between vessels and nerves on the ventral side of the Achilles and chronic tendon pain.9,–,11
The aims with this study were to evaluate the clinical results of the ‘scraping’ technique on a larger group of patients with different activity levels, and also in a randomised study to compare the results of two different scraping techniques (open scraping with a scalpel and percutaneous scraping with a needle).
Material and methods
Patients
Altogether, 103 patients, 66 men and 37 women, mean age 43 years (range 24–77) with midportion tendinosis in 125 Achilles tendons were included. This included 88 tendons as well as 37 tendons in a randomised study. All were treated with a US and colour Doppler (CD)-guided surgical approach outside the ventral tendon. Patients were primarily referred from general practitioners in the northern part of Sweden and from team doctors, to the Sports Medicine Unit in Umeå for a chronic (>3 months' duration of symptoms) painful Achilles tendinopathy, and diagnosed (clinically and by US) to have chronic painful midportion Achilles tendinosis.
Activity level groups
Walking
Twenty-nine tendons in 24 patients (8 males and 16 females, mean age 53 years—range 35–70).
Recreational sports
Twenty-nine tendons in 25 patients (18 males and 7 females, mean age 45 years—range 36–65).
High recreational level
Nine tendons in six male patients (mean age 46 years—range 35–65).
Elite athletes-high national to international level
Twenty-one tendons in 17 patients (14 males, 3 females, mean age 29 years, range 23–36). Track and field (n=7), soccer (n=3), rugby (n=2), cricket (n=2), triathlon (n=1), orienteering (n=1), tae kwon do (n=1).
Randomised study
This study included 31 consecutive patients (elite-level athletes excluded) with midportion tendinosis in 37 Achilles tendons.
Mini-open surgery group
Fifteen patients (10 males and five females, mean age 46 years, range 31–67) with midportion Achilles tendinosis in 18 tendons. Males mean height 181 cm and weight 87 kg, females mean height 170 cm and weight 70 kg. Duration of symptoms 74 months (mean) (range 7–240). Activity levels: jogging (n=7), walking (n=6), skiing (n=1), floor ball (n=1).
Percutaneous mini-surgery group
Sixteen patients (10 males and six females, mean age 47 years, range 31–76) with midportion Achilles tendinosis in 19 tendons. Males mean height 179 cm and weight 83 kg, females mean height 167 cm and weight 69 kg. Duration of symptoms 82 months (mean) (range 5–240). Activity levels: jogging (n=7), walking (n=4), aerobics (n=3), badminton (n=1), floor ball (n=1).
All patients had tried rest from heavy Achilles tendon-loading activities (>3 months), 21 patients had tried anti-inflammatory medication, and 29 patients had tried training programmes including eccentric calf-muscle training, without any effects. No patient had received any injection into the tendon.
There were no significant differences in age, weight, height and duration of symptoms between the patients in the two groups.
Methods
All tendons were examined with high-resolution grey-scale US and CD, Acuson Sequoia (Siemens) at inclusion. A linear multifrequency (8–13 MHz) probe was used. CD was used to diagnose regions with high blood flow, and to locate where the blood flow entered the tendon. Both Achilles tendons were examined.
Large group (88 tendons)
All patients were treated with mini-open surgery using a scalpel, as described below.
Randomised study (31 patients—37 tendons)
The patients participating in the randomised study were allocated to either of two different techniques for surgical scraping.
For both groups
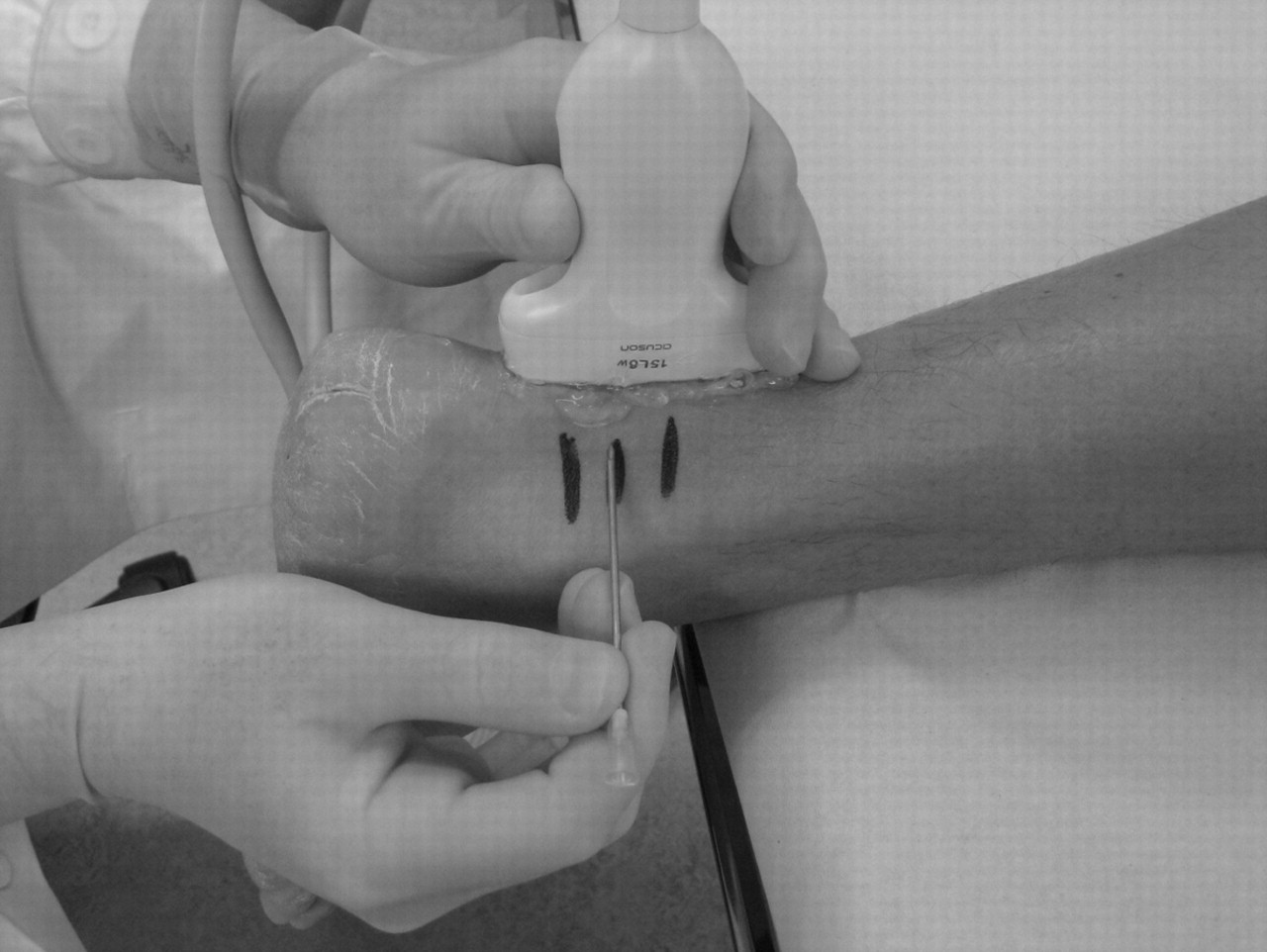
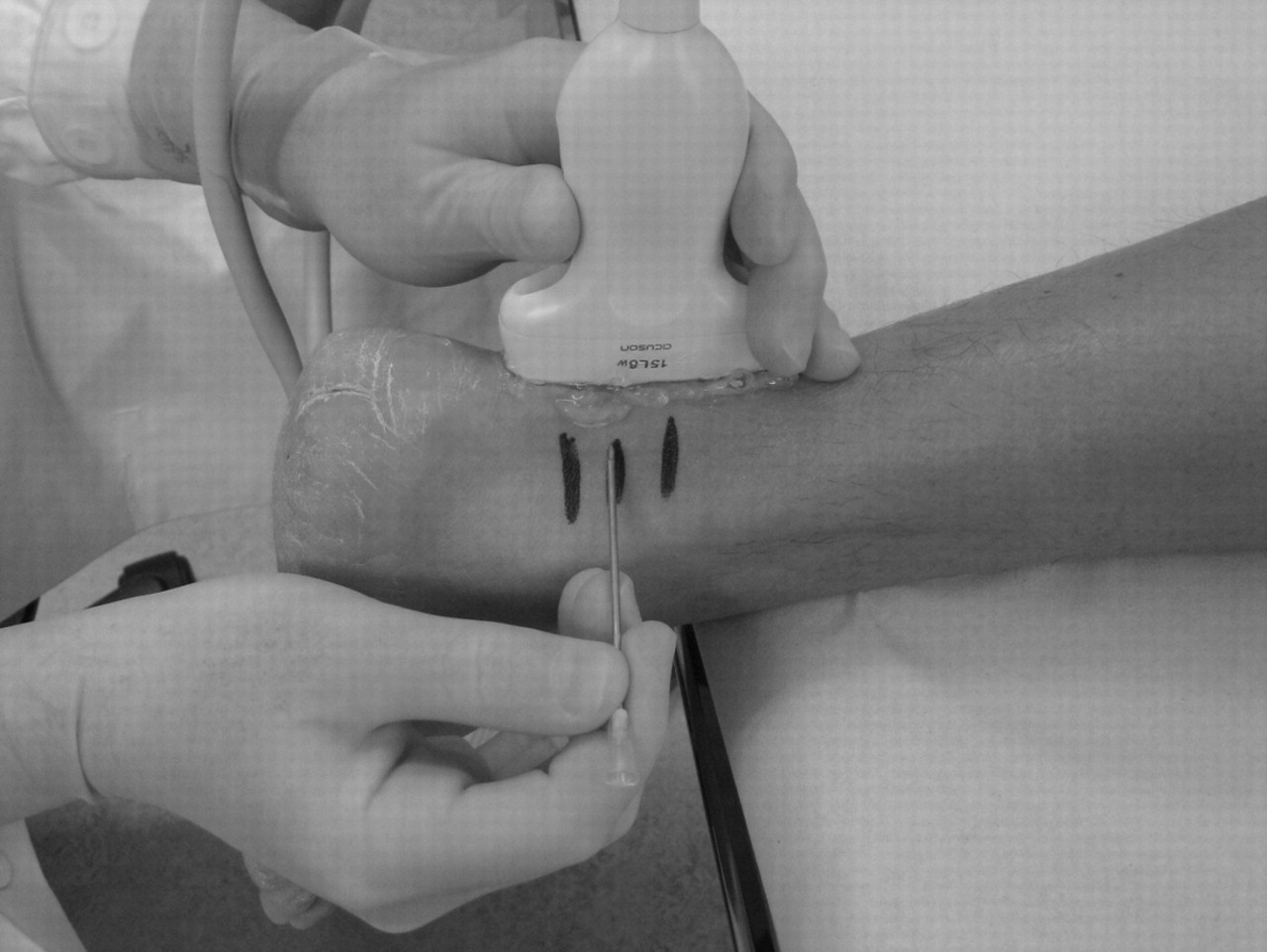
Using US and CD, the structurally abnormal regions with high blood flow inside and outside the ventral Achilles were marked on the skin using a skin marker (figure 1). After washing, a local anaesthetic (5–10 ml of xylocain and epinephrine, 5 mg/ml) was injected on the lateral and ventral side of the Achilles midportion. The skin was then draped with a sterile paper-cover exposing only the midportion of the Achilles tendon.

Ultrasound and colour Doppler examination, used to visualise the tendon and regions with high blood flow, to guide the surgical procedure. The regions with high blood flow inside and outside the structurally abnormal ventral Achilles were marked on the skin by a skin marker.
Mini-open surgery: scraping with a scalpel
A longitudinal skin incision (1–2 cm) was placed on the lateral side of the Achilles midportion, the sural nerve was kept aside and the tendon was carefully identified (figure 2). In the region with tendon changes and high blood flow (marked by skin markers) the tendon was completely released from the ventral soft tissue, by sharp dissection with a knife, staying close to the ventral tendon. This was followed by haemostasis, using diatermia. The skin was closed by single non-resorbable sutures.

Mini-open surgical-scraping with a scalpel. A straight longitudinal skin incision (1–2 cm) was placed on the lateral side of the Achilles midportion.
Percutaneous mini-surgery: scraping with a needle
Using US guidance, a 14-gauge needle was inserted from the medial or lateral side (depending on location of changes), avoiding contact with the sural nerve (figure 3). Keeping the needle close to the ventral side of the tendon, the region with tendon changes and high blood flow was released from the ventral soft tissue by scraping with the sharp side of the needle, staying close to the ventral tendon.
{kind=link}
{kind=link}
{kind=link}
Percutaneous mini-surgical scraping with a needle. Ultrasound was used to guide the insertion and scraping, where a 14-gauge needle was inserted ventral to the tendon, from the medial or lateral side (depending on the location of the changes).
Rehabilitation: all patients
Day 1: rest, elevated foot. Day 2, ROM exercises, light stretching and short walks. Day 3–7: gradually increased walking activity. Day 8–14, light bicycling. After 2 weeks: sutures out, gradually increased load up to free activity on pain and depending discomfort.
Follow-ups
The majority of patients were followed up clinically and by US and CD at 6, 12, 26 and 52 months postoperatively. Long-distance patients were followed up by telephone or mail.
Outcome measures
Pain during Achilles tendon-loading activity
The patients recorded tendon pain during their activity (walking, recreational sport, high-level sport), before and after treatment, on a 100 mm long Visual Analogue Scale (VAS), where no pain was recorded as 0 and severe pain as 100.
Patient satisfaction with the result of the treatment was determined by self-reporting (satisfied or not satisfied).
Ethics
Ethical approval was obtained from the Ethical Committee at the Medical Faculty of the University of Umeå.
Statistical methods
Results are presented as mean and range values.
Randomised study
The Wilcoxon signed ranks test was used to study the differences in VAS, before and after treatment, in each group.
Results
Before surgery, all patients were unable to participate in Achilles tendon loading activity without pain. The mean VAS was 77.
After surgery (follow-up mean 18 months, range 6–33) there was a good clinical result in 111 tendons (89%), with satisfied patients back in full Achilles tendon loading activity. The mean VAS during the Achilles tendon loading activity had decreased significantly from 77 to 2 (p<0.005).
Results in the different activity-level groups
Walking
Follow-up >1 year in 23/29 patients (range 6–31 months). Satisfied: 23/29 tendons—18/24 patients. Not satisfied: five females and one male.
Recreational sports
Follow-up >1 year in 14/25 patients (range 7–24 months). Satisfied: 28/29 tendons—24/25 patients. Not satisfied: one female.
High recreational level
Follow-up >1 year in 4/6 patients (range 6–15 months). Satisfied: 9/9 tendons—6/6 patients.
Elite athletes: high national to international level
Follow-up >1 year in 13/17 patients (range 7–20 months). Satisfied: 21/21 tendons—17/17 patients.
Randomised study
Mini-open surgery with a scalpel
Before surgery, the mean VAS during Achilles tendon loading activity was 69 (range 40–92). After surgery, there was a good clinical result in 15/18 tendons (83%), with satisfied patients back in full Achilles tendon loading activity. The mean VAS during Achilles tendon loading activity had decreased significantly from 69 to 6 (range 0–38; p<0.005). In 3/18 tendons, there was a poor clinical result, with patients not being satisfied and having Achilles tendon pain during activity. Their VAS was 92, 80 and 35, respectively.
Percutaneous mini-surgery: scraping with a needle
Before surgery, the mean VAS during Achilles tendon loading activity was 75 (range 40–99). After surgery, there was a good clinical result in 15/19 tendons (74%), with satisfied patients back in full Achilles tendon loading activity. Their mean VAS during Achilles tendon loading activity had decreased significantly from 75 to 2 (range 0–15; p<0.005). In 4/19 tendons, there was a poor clinical result, with patients not being satisfied and having Achilles tendon pain during activity. Their VAS was 100, 90, 82 and 69, respectively.
There were no significant differences in the mean VAS during the Achilles tendon loading activity between mini-open treatment with a scalpel and percutaneous treatment with a needle.
Complications
One wound infection, one wound rupture and one partial Achilles tendon rupture (related to a major trauma).
Discussion
This prospective study on a large group of patients with chronic painful midportion Achilles tendinosis evaluated surgical ‘scraping’ outside the ventral Achilles midportion, including a randomised study evaluating two different surgical techniques. Good clinical results were obtained in 89% of the patients, and the randomised study showed no differences between open scraping with a scalpel and percutaneous scraping with a needle.
This new surgical approach used in this study was based on recent findings from tendon tissue specimens taken from the region with US and CD verified tendon changes and high blood flow inside and outside the ventral Achilles midportion.9 Immunohistochemical analyses showed few nerves inside the tendon but several in close relation to blood vessels outside the ventral Achilles midportion.10 11 Recent studies using sclerosing polidocanol injections, targeting the region with blood vessels and nerves outside the ventral Achilles, showed good clinical results.2 3 14 This one-stage, more radical, mini-surgical scraping technique targets the region with high blood flow (blood vessels and nerves) outside the ventral Achilles tendon is subjected to the surgical scraping.
Interfering with the tendon blood supply by ‘scraping’ on the ventral side of the Achilles did not appear to have a negative effect on the tendon blood flow. Importantly, only the regions with changes, and not the whole ventral tendon, was ‘scraped.’ It is essential to use US and Doppler to identify carefully blood flow and tendon abnormality.
In the current study, we grouped the patients in relation to their activity levels. Interestingly, the results after treatment were best in the high-activity groups, such as elite-level athletes, and not similarly good in the low activity group. These results might indicate that the tendon needs to be loaded for an optimal response to this treatment. We used a fairly quick return to activity after treatment, with walking in the first week and biking second week, followed by a gradual return to full tendon loading activity in most patients within 4–6 weeks. This postoperative rehabilitation regimen seems to work well in the majority of the patients; a few patients in the low activity group needed a longer period to return to full activity. Also, the low-activity group were older than the high-activity group (53 years old compared with 29 years old). However, the recreational activity groups that also had good clinical results had a similar mean age (45 and 46 years, respectively). Six of the eight women who had a poor result with treatment were found in the low-activity group. Interestingly, in a previous study of patients with midportion Achilles tendinosis treated with eccentric training, the majority of the patients with a poor result of the treatment were females.1 Maybe females, at least in this age group (mean 56 years), respond less well to these treatments.15 In future studies, it would be of interest to study if there are any gender-dependent differences in the response to different types of treatment.
A limitation of the current study was that many patients lived long distances away from our clinic, and not all patients were followed up by clinical examination and US and Doppler examination. Instead, these patients were contacted by mail or telephone. Only athletes back in full pain-free training and competition were considered to have good results in response to treatment. Another limitation in the study is that we did not record the weight and height for all patients. Also, the follow-up period after surgery was not long, and there could be more failures with time. However, patients with poor results after treatment were found early, the majority within 6 months, and none later than 1 year after the operation.
In conclusion, US and Doppler-guided ‘scraping,’ open with a scalpel or percutaneous with a needle, has shown good clinical short-term results and few complications in patients on different activity levels. Ongoing studies should focus on the longer-term clinical results and effects on tendon thickness and structure. A fast pain relief and return to even high level sports activity seems possible with this treatment approach.
What is already known on this topic
It is known that there are blood vessels and nerves on the ventral side of the chronic painful Achilles tendinosis tendon, and that two or three treatment sessions of US- and Doppler-guided injections with the sclerosing substance polidocanol, targeting the region with blood vessels and nerves outside the ventral tendon, can cure the tendon pain.
What this study adds
This study shows that the one-stage procedure US and Doppler-guided mini-surgical scraping, targeting the region with blood vessels and nerves outside the ventral tendon, can cure the tendon pain and allow for a relatively rapid return to full Achilles tendon loading activities with a low risk for complications.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the Ethics Committee Umeå University.
-
Provenance and peer review Not commissioned; not externally peer reviewed.